
Chapter 16: The good casualty officer
A 21-year-old woman went to the emergency department worried that she was getting short of breath over the last 2 weeks and now could not even climb up the stairs at home. She had no chest pain or cough. Her last menstrual period was 4 months ago but she had had intermittent irregular heavy vaginal bleeding since then.
She had a sinus tachycardia (90 per min) and was hypotensive (100/60 mmHg). Her resting respiratory rate was 25 per min.
Just before sending her for a chest X-ray, the casualty doctor did a urinary pregnancy test which was positive. Instead of sending her for a CXR, the doctor requested a transvaginal ultrasound and a quantitative serum HCG which was 100,000 IU/L.
-
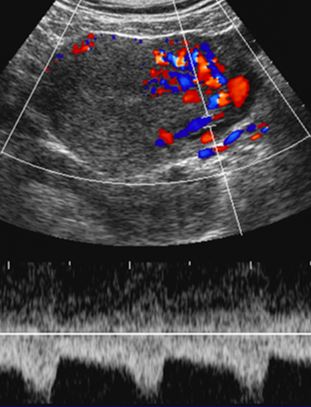
1. What does the transvaginal ultrasound show?
Correct answer:
Transvaginal ultrasound shows an enlarged uterus but no foetus. The uterus contains a hyperechoic mass containing many cysts with increased vascularity on Doppler studies. The appearances are due to a complete mole (gestational trophoblastic disease).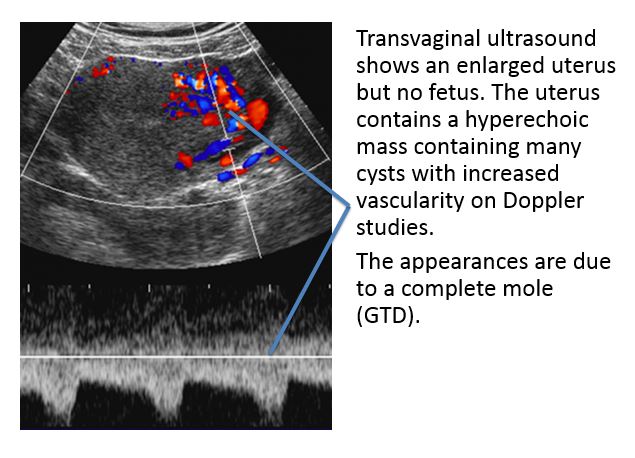
-
2. What features characterize a complete hydatidiform mole?
The majority of complete moles have a 46XX karyotype, with both X-chromosomes of paternal origin (androgenetic). They are believed to originate from fertilization of an empty ovum by a haploid sperm that then underwent duplication.
-
3. How are serum human chorionic gonadotropin (HCG) measurements used in the clinical management of gestational trophoblastic disease?
Staging investigations confirmed that she had pulmonary metastases. According to the WHO/FIGO prognostic scoring system, she had low risk disease. She was therefore treated with single agent methotrexate chemotherapy. The patient was cured, thanks to the good casualty doctor who wisely decided on a career in medical oncology.