
Chapter 14: The Rasta with a backache
A 67-year-old Jamaican Rastafarian complained to his general practitioner of lower back ache and was referred to an orthopaedic surgeon. As he was tender over L2 vertebra, the orthopaedic surgeon arranged a bone scan and an MRI scan.
-
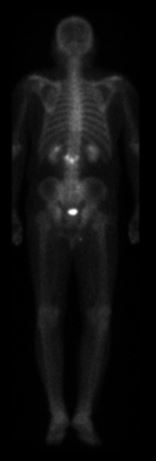
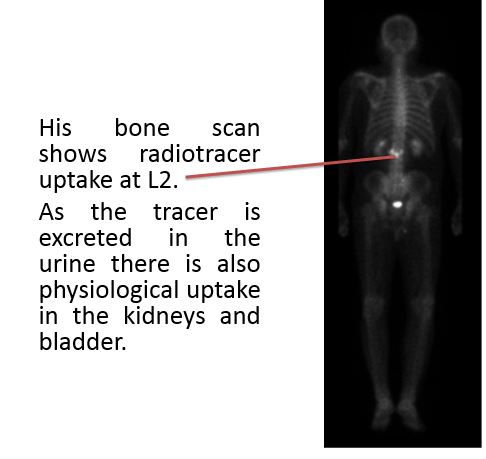
1. What does the technetium pyrophosphate radionuclide bone scan show?
Correct answer:
An MRI was done.
-
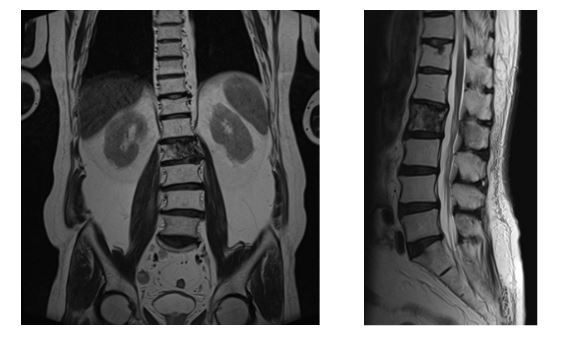
2. What does the MRI scan show?
Correct answer:
His bone scan shows radiotracer uptake at L2 and MRI demonstrates a destructive lesion in L2 with no cord compression.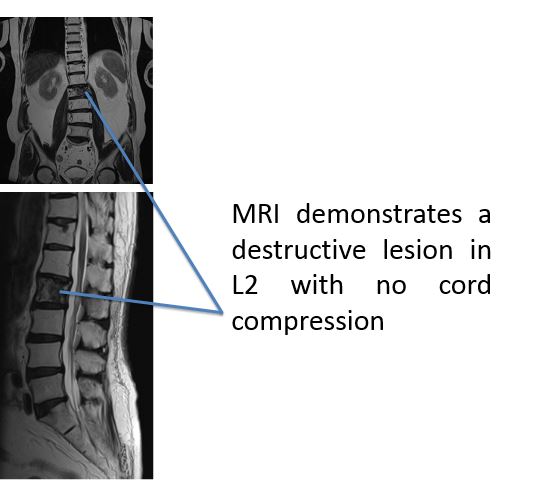
The surgeon is concerned that he is at risk of cauda equina compression and he performs a lumbar spine stabilization surgery using pedicle screws. He sent some of the bones for histological analysis.
-
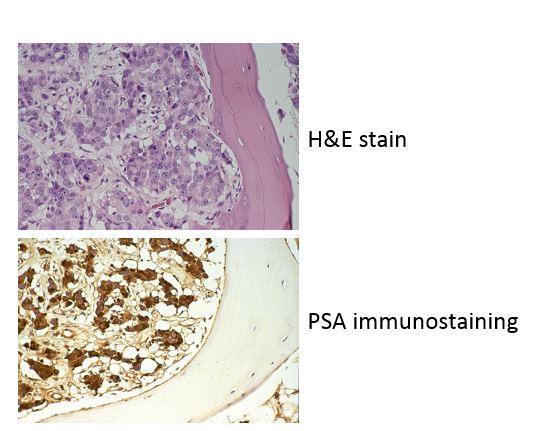
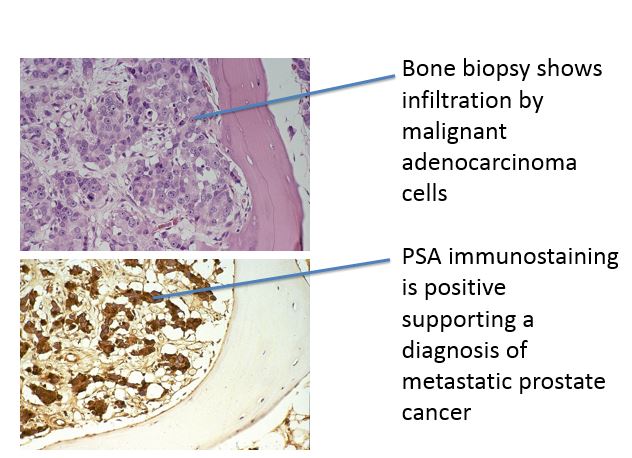
3. What does the bone biopsy show?
Correct answer:
-
4. How could the surgeon have worked out the diagnosis easier?
-
5. If the normal range of PSA used in screening programmes was raised from 4 μg/L to 6 μg/L, what would be the effect on sensitivity, specificity, false positive and false negative rates?
Following surgical fixation, our patient had a serum PSA which was 128 μg/L and a TRUS biopsy confirmed prostate cancer Gleason grade 4+5. He was treated with maximal androgen blockade, a combination of an antiandrogen (bicalutamide) and a gonadotropin-releasing hormone agonist (goserelin acetate). His prognosis of a median survival is around 6 years.