
Chapter 12: A heart of gold and an oncocytoma
A 56-year-old housewife complained of chronic pelvic pain to her GP who knew her well. She was from Preston and had married well and moved to a fashionable area of London. She knew everyone in the street and all their business and was always quick with advice. As she was insured her GP referred her to a gynaecologist who arranged imaging of her abdomen and pelvis.
-
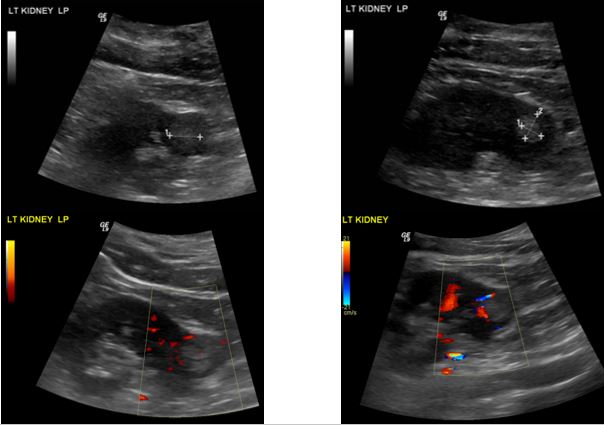
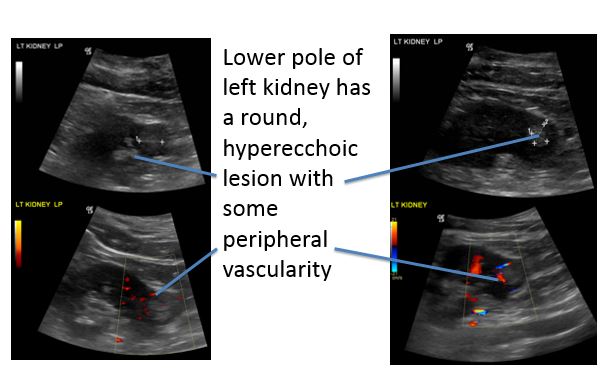
1. What does the abdominal ultrasound show?
Correct answer:
Lower pole of the left kidney has a round, hyperechoic lesion with some peripheral vascularity. In view of these findings she has a CT urogram.
-
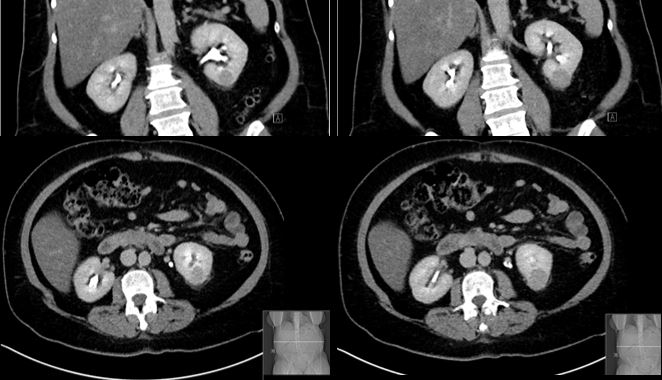
2. What does the CT urogram show?
Correct answer:
Exophytic mass at the posterior aspect of the inferior pole of the left kidney, with a mean of 18 Hounsfield units. This mass enhances heterogeneously with contrast and is keeping with a renal tumour.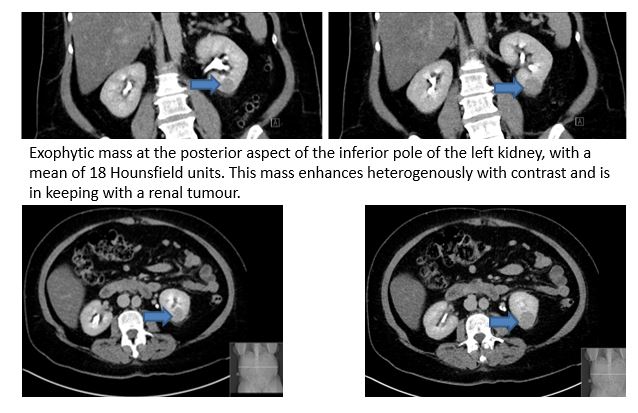
-
3. What features on a CT scan suggest that a kidney cyst is cancerous?
-
4. What is the classic triad of features at presentation suggesting a diagnosis of renal cancer?
This triad is only found in 10% cases.
-
5. What non-metastatic manifestations of malignancy occur in renal tumours?
About a quarter of patients present with metastatic disease.
-
6. What are the most common sites for secondary spread in kidney cancer?
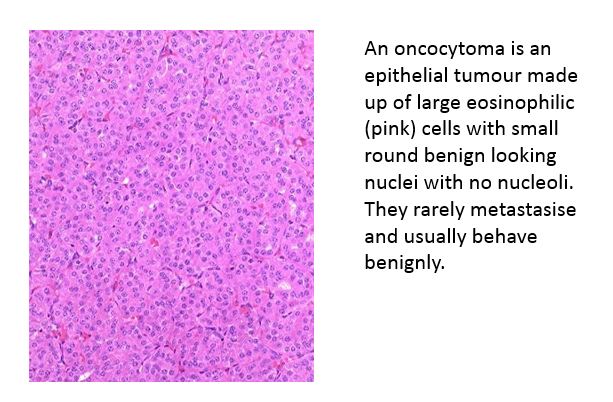
She had a laparoscopic nephron-sparing partial nephrectomy for a stage I (pT1N0M0) oncocytoma. An oncocytoma is an epithelial tumour made up of large eosinophilic (pink) cells with small round benign looking nuclei with no nucleoli. They rarely metastasize and usually behave benignly.
She had no post-operative adjuvant treatment as even in the much more common and more aggressive renal cell carcinoma, no adjuvant treatment whether it be radiotherapy to the renal bed, chemotherapy, chemo-immunotherapy, cytokine therapy or anything else has been shown to be beneficial after surgery.
Her pelvic pain did not improve and she also complained of back pain and headache that she attributed to epidural analgesia; also the NHS hospital food was not up to much and the staff were much friendlier in the hospitals up North where she had delivered her children.