
Chapter 9: The co-infected CÔte d’Ivorian
A 37-year-old man from Cote d’Ivoire presented with abdominal pain and swelling and mild dyspnoea. He was known to have HIV since 2003 and was on anti-retroviral therapy (truvada, darunavir, ritonavir) with a CD4 count of 457/mm3
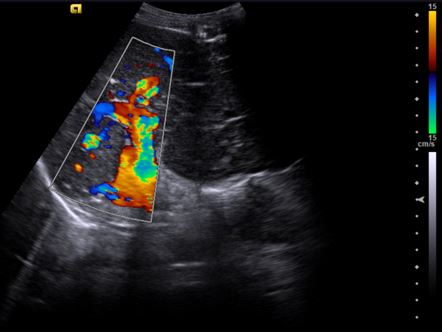
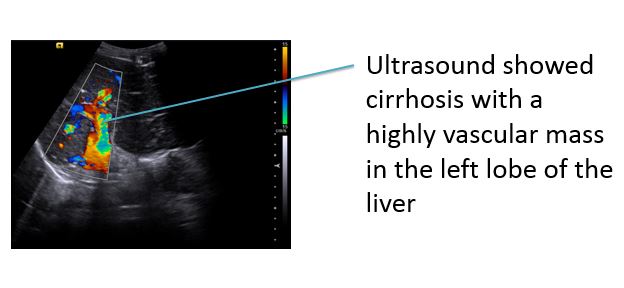
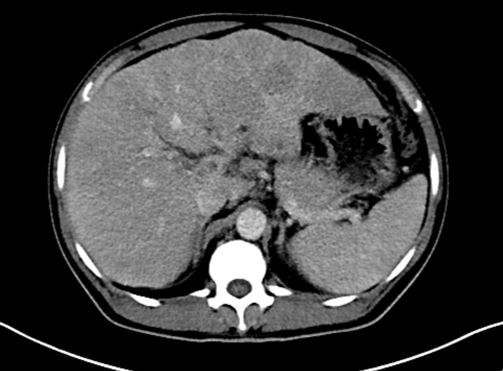
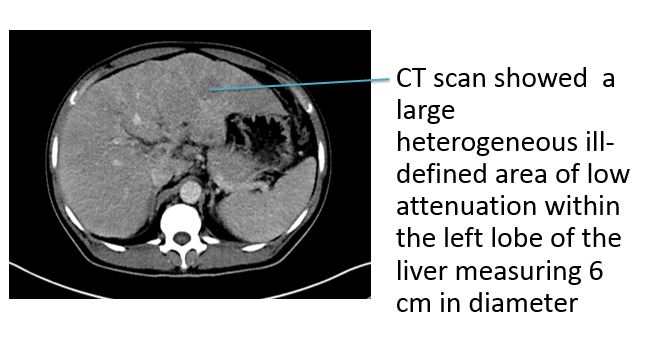
1. Who should be screened for liver cancer and what screening should be undertaken? 2. What does the liver ultrasound show? Correct answer: 3. What does the CT scan show? Correct answer: Ultrasound showed cirrhosis with a highly vascular mass in the left lobe of the liver. CT scan showed a large heterogeneous ill-defined area of low attenuation within the left lobe of the liver measuring 6 cm in diameter. As the tumour was greater than 5cm in diameter it was not suitable for surgical resection. The current criteria for curative surgical resection are: single tumour <5 cm diameter or up to three tumours all <3 cm diameter. 4. What infections are implicated in the pathogenesis of hepatic and biliary tumours? As he has advanced hepatocellular cancer he is offered palliative treatment with sorafenib, a receptor tyrosine kinase inhibitor that is associated with a modest but significant increase in time to disease progression. Fortunately his oncologist consults his HIV physician first as there are significant drug interactions between the sorafenib and the antiretrovirals. The ritonavir will reduce the metabolism of the sorafenib potentially leading to toxic levels. Conversely, the sorafenib could lead to raised and potentially toxic levels of raltegravir, one of the likely alternative antiretrovirals. Knowledge of pharmacokinetics is essential when prescribing systemic anticancer therapy. Sorafenib could raise raltegravir levels as it is metabolized by UGT1A1.