
Chapter 37: A tired retired engineer
A retired engineer aged 83 years went to see his GP because he was lethargic. He admitted to 10 kg weight loss and vague right upper quadrant fullness.
He was an ex-smoker (25 pack years). There was no family history of cancer or occupational carcinogen exposure. He was on no medication and had no significant past medical history.
His GP referred him to a gastroenterologist who organized a CT scan and various blood tests.
| Serum calcium (adjusted) | Result | Normal range |
|---|---|---|
| Serum calcium (adjusted) | 3.20 (3.45) mmol/L | 2.15-2.60 |
| Albumin | 21 g/L | 35-50 |
| Phosphate | 1.28 mmol/L | 0.8-1.5 |
| Alkaline phosphatase | 417 IU/L | 30-130 |
| Alanine transaminase | 57 IU/L | 0-40 |
| Bilirubin | 39 mcmol/L | 0-21 |
| AFP | 3 kU/L | 0-13 |
| CEA | 5 mcg/L | 0-5 |
| CA12-5 | 3756 U/mL | 0-35 |
| CA19-9 | 5536 U/mL | 0-33 |
| PSA | 0.23 mcg/L | 0-4 |
Abdominal CT scan.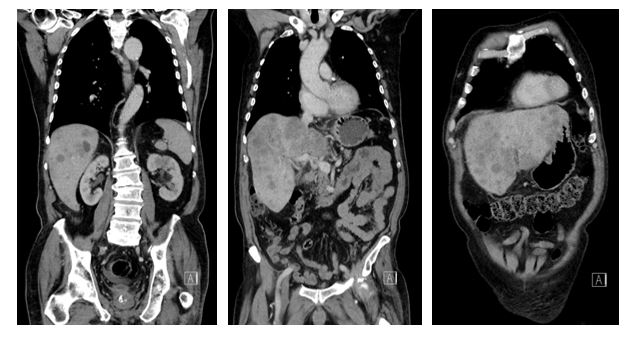
-
1. What does the abdominal CT scan show?
Correct answer:
CT scan shows hepatomegaly with multiple liver metastases.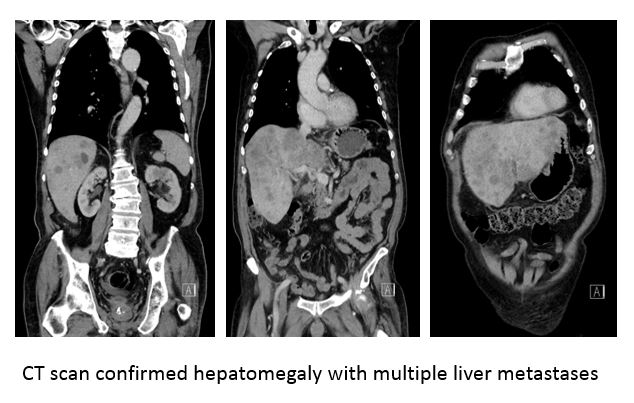
Thoracic CT scan.

-
2. What does the thoracic CT scan show?
Correct answer:
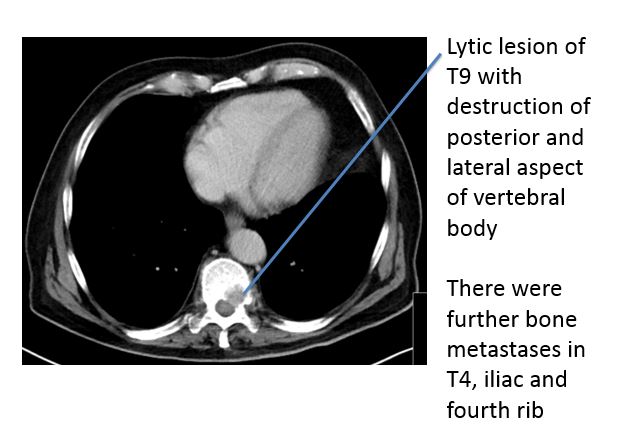
Lytic lesion of T9 with destruction of posterior and lateral aspect of vertebral body. There were further bone metastases in the T4, iliac and fourth ribs.
He had a diagnostic ultrasound-guided liver biopsy.
| Liver biopsy report |
| Microscopic description: |
| Liver infiltrated by an undifferentiated carcinoma with focal packaging but no definite evidence of glandular differentiation. |
| Immunohistochemical staining: |
| The tumour is diffusely positive for CK7, CK20 and CK19 and CDX2. |
| It is negative for chromogranin and CK5. |
| This immunophenotype is not specific but indicates that the tumour is a poorly differentiated adenocarcinoma. |
-
3. What are the most common primary tumour sites in patients with liver metastases?
Although his gastroenterologist suspected an upper GI primary or pancreatobiliary primary, no primary was present on the CT scan and an upper GI endoscopy was unremarkable.
He was treated for hypercalcaemia of malignancy with rehydration and zoledronate and declined palliative chemotherapy. He died 1 month later at home as this was his preferred place of death, having received excellent community-based palliative care from his local hospice.