
Chapter 33: The Chelsea pensioner with a leg ulcer
An 83-year-old Chelsea pensioner presented with a pigmented bleeding ulcerated lesion on his left lateral lower leg. The surgeon apothecary (lieutenant colonel) referred him to a dermatologist.
-
1. What features of a pigmented skin lesion should arouse suspicion?
An excision biopsy confirmed a diagnosis of malignant melanoma 2.8 mm deep (Breslow’s depth IV) invading into the reticular dermis (Clark’s level 4). The tumour showed vertical growth phase with frequent mitoses (>5/mm2). <AU: Please check the unit in “>5/mm2”.>Molecular analysis showed that the tumour lacked the BRAF v600 mutation.
Staging investigations suggested no local or distant spread (T3bN0M0 stage 2B).
A further wider excision with a 3 cm margin and skin grafting was performed. No adjuvant therapy was given.
-
2. What is the significance of the lack of BRAF v600 mutation?
Correct answer:
Patients whose tumours have the V600 mutations of the BRAF gene are candidates for treatment with the BRAF inhibitors vemurafenib and dabrafenib. If the tumour has wild-type BRAF, treatment with ipilimumab that targets CTLA-4 is appropriate. However, neither is used in the adjuvant context.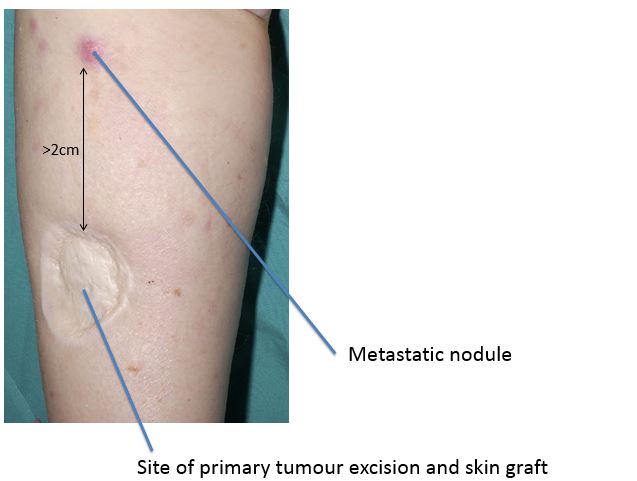
After 6 months he developed a skin nodule >2 cm distant from the original tumour site but before the regional lymph nodes. Surgical excision of the nodule confirmed metastatic melanoma.
-
3. What term is applied to this form of spread?
After 4 months he noticed a lump below the skin on his flank.

-
4. What does the CT scan show?
Correct answer:
CT shows a subcutaneous metastasis which was excised by a plastic surgeon.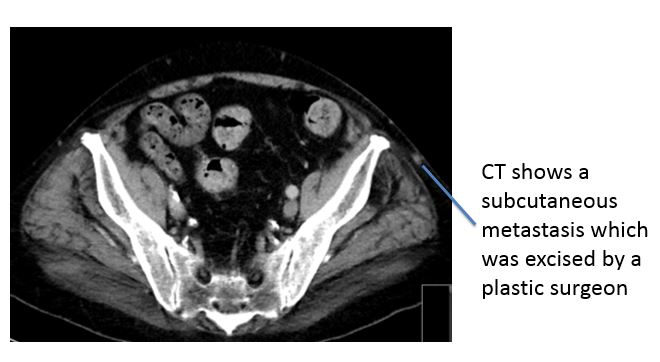
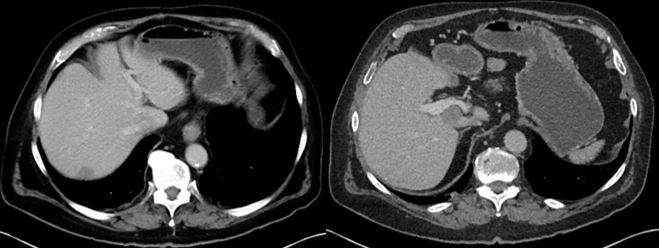
Just 2 months after this he complained of fatigue.
-
5. What does the CT scan show?
Correct answer:
The CT scan shows multiple liver metastases.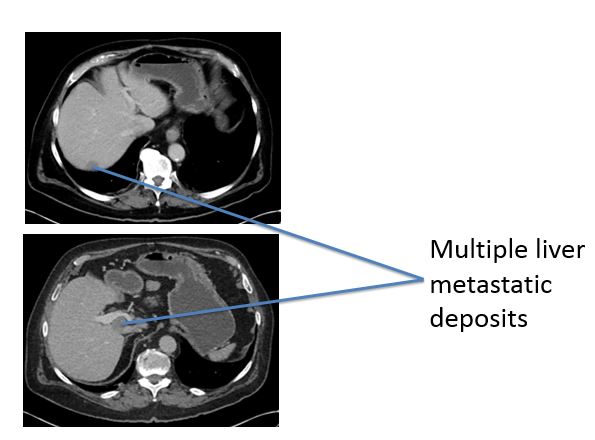
He declined therapy with ipilimumab after he read in the Daily Mail that it only extends life by 4 months on average and costs £75,000 per person. He did ask his oncologist if he could have the money instead though.