
Chapter 30: The Eritrean woman with a swollen jaw
A 22-year-old woman from Eritrea presented with a rapidly enlarging lump on the side of her face. Over the last fortnight she had developed night sweats and fevers.

She is referred by her GP to an ENT surgeon who suspects a non-Hodgkin’s lymphoma (NHL).
-
1. What are the most common subtypes of NHL?
After nasendoscopy to exclude an aerodigestive primary, she has a lymph node excision and bone marrow aspirate and trephine biopsy.
-
2. What does her bone marrow biopsy show?
Correct answer:
Her bone marrow is almost completely replaced by an infiltration of small non-cleaved abnormal lymphocytes of Burkitt’slymphoma. This is confirmed by immunostaining for CD20, CD10 and K67 (MIB-1).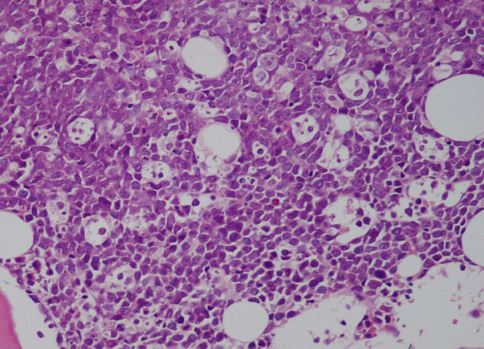
-
3. What chromosomal translocation is associated with Burkitt’slymphoma?
-
4. What stage disease does she have?
A final diagnosis of stage IVB Burkitt’slymphoma was made. Her HIV serology was negative. She was treated with two cycles of alternating R-CODOX-M/R-IVAC intensive chemotherapy and intrathecal chemotherapy prophylaxis. Each cycle was complicated by febrile neutropenia despite prophylactic G-CSF. She achieved a complete radiological remission confirmed by PET-CT imaging.