
Chapter 26: A charlady with a rash
A 67-year-old non-smoking charlady became very breathless. She had had a cough for a month and some pain over the left side of her chest when she coughed.
-
1. What symptoms and signs require urgent referral for suspected lung cancer?
Her GP sends her straight to the emergency department where she has a chest X-ray.

-
2. What does the chest X-ray show?
Correct answer:
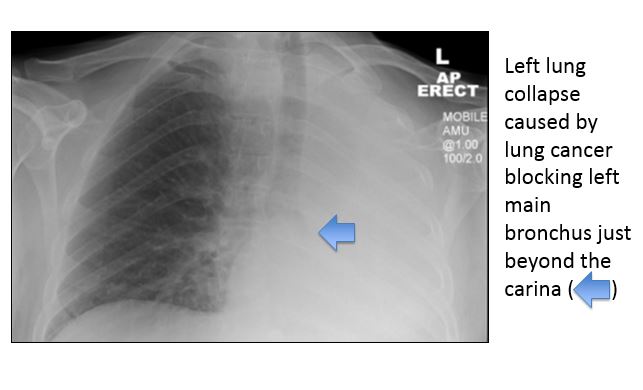 Left lung collapse caused by obstruction to the left main bronchus.
Left lung collapse caused by obstruction to the left main bronchus.
A bronchoscopy is arranged that reveals a tumour occluding the left main bronchus.
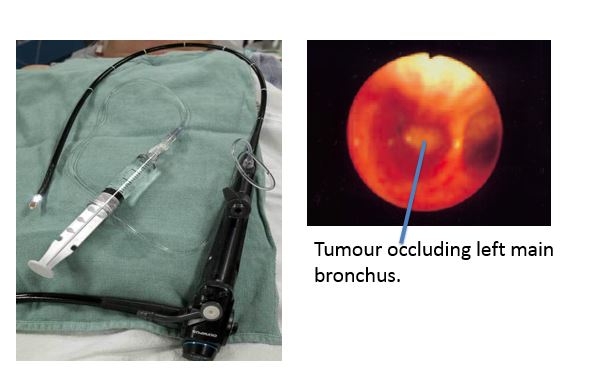
Bronchoscopic biopsy showed adenocarcinoma and staging of the tumour confirmed T3N0M1a disease with metastases in the contralateral lung.
-
3. What is the most common histological type of lung cancer amongst non-smokers?
Molecular analysis was performed on the primary tumour which showed that the cancer had an exon 19 deletion in the epidermal growth factor receptor (EGFR). The optimum treatment for adenocarcinoma of the lung is determined by the molecular signature. Tumours with inactivating mutations of EGFR may be treated with oral tyrosine kinase inhibitors such as erlotinib and gefitinib. Tumours with the rarer anaplastic lymphoma kinase (ALK) gene rearrangement or fusion are also associated with adenocarcinomas in younger non-smokers and often signet ring or acinar histology. These tumours may be treated with crizotinib, an oral tyrosine kinase inhibitor that targets ALK.
She was treated with erlotinib therapy following endoscopic stenting of the left main bronchus. One month into erlotinib treatment she developed this severe rash. The erlotinib rash is often associated with tumour responsiveness.
